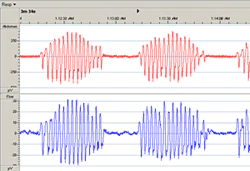
CSR occurs when periods of hyperventilation and hypoventilation, in a waxing and waning breathing pattern, alternate with periods of central hypopnea and apnoea.
CSR has been found to be a highly prevalent form of SDB in patients with severe left ventricular dysfunction.3